Patients | General Information
Obstructive Sleep Apnea
Sleep Apnea
Obstructive sleep apnea (OSA) has only recently been recognized as a significant health problem. It is estimated that 4-6% of adults are affected. The incidence increases greatly with age and obesity. For years patients with loud snoring have been the object of ridicule and jokes. Sleep apnea is no joke. The incidence of many serious health problems have been directly linked to OSA (Table 1).
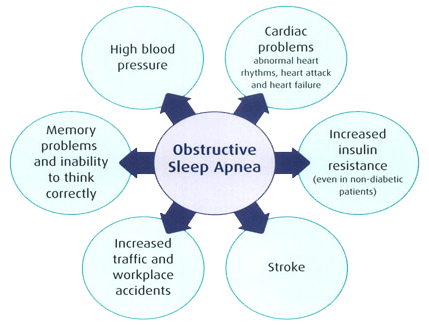
Table 1
Health problems related to OSA
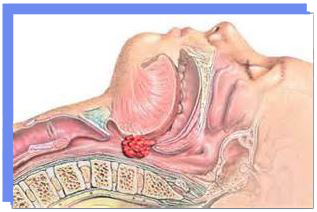
What is obstructive sleep apnea? During wakeful hours healthy people are able to maintain their breathing passage without any problem. However, during sleep the body relaxes and tissue in the mouth and throat can collapse causing obstruction. Obstructioin can occur from the tip of the nose down to the back of the tongue and voice box. (see Figure 1). As the tissue collapses further there is a suction effect that causes further collapse much the same as occurs when you suck on a narrow straw. If this occurs more than 5 times an hour you are diagnosed with OSA. As the number of events increase the symptoms and associated risks increase.
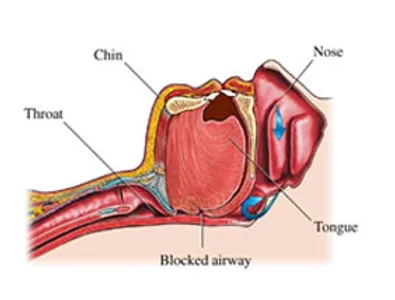
Figure 1
How do I get tested? The evaluation for sleep apnea begins with a visit to your doctor. A questionnaire (the Epworth Sleepiness Scale) may be administered in order to determine if you are at risk for OSA. The gold standard diagnostic test is an over-night sleep study (polysomnogram). Your doctor will receive a report grading your study as normal or indicating sleep apnea (mild, moderate, or severe). If you do have OSA you will be called back to the lab for a trial of continuous positive airway pressure (CPAP). The CPAP device forces air past the tissue that is obstructing your airway.
What are the treatments? CPAP has long been the gold standard for the treatment of OSA.
For those patients who do not tolerate CPAP there are alternative. The sleep lab will make every effort to try different custom masks and different air pressure algorithms (continuous or biphasic). Some people (20-50%) are unable to adjust to PAP. Fortunately there are options (Table 2).

Nasal CPAP

Table 2
Alternatives to CPAP

Mandibular Advancement Devices
The treatment options always begin with conservative treatment. The next step is the use of either mandibular advancement devices (seen above) or tongue retention devices.
For patients with severe obesity (BMI >40) Bariatric surgery offers an opportunity to both lose weight and improve obstructive sleep apnea. In rare cases of severe life threatening OSA a tracheostomy may be recommended. Although tracheostomy is rarely performed as a long term solution for OSA, it does have a cure rate of 100%. Tracheostomies are readily reversible should a patient lose weight or undergo other surgery to address OSA.
The surgical treatment of sleep apnea is varied depending on the site and nature of the obstruction. For patients with a recessive jaw (retrognathia) the best option is a bi-maxillary advancement (moving the upper and lower jaw forward) which is performed by oral and maxillofacial surgeons. For all other types of obstruction surgery is typically performed by an otolaryngologist. The key to successful surgery is to identify and address the site(s) of obstruction before surgery.
Sleep endoscopy allows the surgeon to examine the patient’s airway during drug induced sleep using a small fiberoptic scope inserted through the nose. This procedure helps to identify hidden areas of obstruction that may not have been recognized during the office examination. Most patients have obstruction in the area of the palate, tonsils (if present) and the back of the tongue (lingual tonsils and epiglottis). After sleep endoscopy the patient and his or her family are given the opportunity to review video of the procedure and discuss options, expected outcomes, and associated risks. A list of commonly performed procedures can be found in information about surgery.
Obstructing Lingual Tonsils
Additional Information
- American Academy of Otolaryngology – https://www.entnet.org/HealthInformation/Surgery-for-Obstructive-Sleep-Apnea.cfm
- Americian Academy of Sleep Medicine – http://yoursleep.aasmnet.org/ and http://www.sleepeducation.com/
- National Sleep Foundation – http://www.sleepfoundation.org/