Patients | Procedures
Epiglottoplasty
 In some cases procedures can be done in different stages; the thyrohyoidopexy is done first followed by a sleep study in three months. If there is residual sleep apnea the palate work can be done later if necessary.
In some cases procedures can be done in different stages; the thyrohyoidopexy is done first followed by a sleep study in three months. If there is residual sleep apnea the palate work can be done later if necessary.
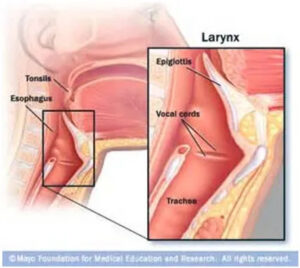
In a small percentage of patients the epiglottis plays a significant role in obstructive sleep apnea. This problem is usually identified when the patient undergoes sleep endoscopy – part of the usual diagnostic workup for patients with sleep apnea. During wakefulness patients have muscle tone that prevents the epiglottis from falling in to the airway. During sleep, however, some patients will experience obstruction due to the epiglottis falling into the airway – the floppy epiglottis.
As part of Trans Oral Robotic Surgery (TORS) the epiglottis may be trimmed. It is important to preserve the protective mechanism of the epiglottis in preventing inadvertent aspiration of food, drink, and saliva. The removal of epiglottic tissue is conservative. Only the upper third of the epiglottis is removed which preserves adequate protection for the patient.
Not all patients have a “floppy” epiglottis. The problem is confirmed at the time of Sleep endoscopy. The risks of epiglottoplasty include temporary cough when eating, a sense that food sticks or hangs up at the base of the tongue that can persist for months. There is no change in voice that accompanies this procedure. In rare cases patients have experienced (food going down the wind pipe) that has required hospitalization for pneumonia and the placement of a temporary feeding tube to prevent further episodes of aspiration during the healing process.